

Have you ever wondered if your organization is capturing 100% of your infusion revenue and capturing charges efficiently? Do you think your organization is using coders effectively to get charges out the door? Are coders required to review every single charge before it goes to billing?
We’ve audited healthcare organizations across the US and found that the majority had significant errors when it came to outpatient infusion coding and billing. Wondering if you might be leaving missed revenue on the table?
Outpatient infusion coding is complex which is why so many healthcare organizations can easily miss out on maximizing their reimbursements if they’re doing the calculations manually.
We can audit a sample of your recent outpatient infusion charges to determine if there are errors prevalent that could’ve been fixed by our Charge Infusion application. Not only would this mean an increase in reimbursement for the same services performed, but it also ensures your billing is completely compliant and in line with your documentation.
Curious if you’re missing revenue or charges? I can take a quick look at your recent infusion charges to help determine if you’re missing any charges or billing things incorrectly. To do this, I ask for:
- 20-30 complete accounts of data
- Clinical documentation related to the infusion services
- Names and types of drugs administered (chemo, hydration or therapeutic) and the route of administration (how the drug was delivered)
- Start and stop times of when the drug was administered
If you find that collecting this information is troublesome, you’re not alone. This information is often stored in multiple places within your EHR or in a pharmacy database, or sometimes not stored at all. But I can help you find this information or use the information you give me to get an estimate of your potential missing revenue.
Below is a basic spreadsheet of data I collected from a customer that shows infusion under-coding which is one major cause of missed revenue. As you can see, I went through each charge and noted why there was missing revenue on the table. In some instances, you can see they were missing stop times, so the code was assigned as an IV push. In others there was missing documentation. The totals in red are the missing revenue this healthcare organization could’ve billed for – but didn’t.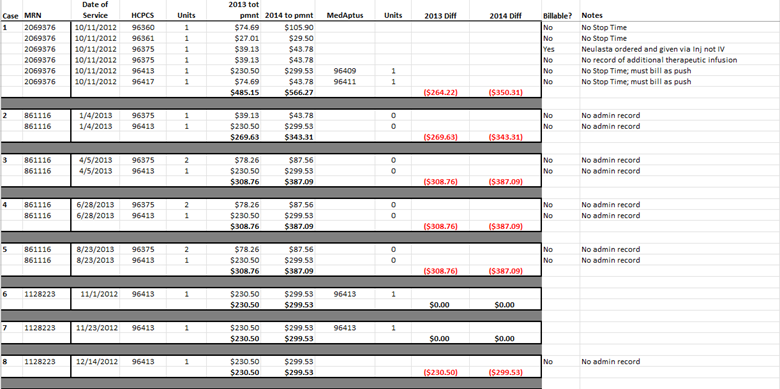
The most common errors I see when auditing outpatient infusion charges are:
- Missing documentation – missing stop times or missing drug identifiers or incorrect drug identifiers.
- Incorrect documentation – a mismatch between what’s billed and what’s documented. This puts you at risk for compliance issues or audits. These errors might look like:
- Rounding down start and stop times to make the math easier to do on the go.
- It is more common for coders to under-code—erring on the side of caution– but this results in missed infusion revenue. And remember, even under coding is not compliant.
- Missing full documentation – ex. emergency department is busy, and someone forgot to put in that they injected an antibiotic drug or performed a hydration IV.
- While administering a complex protocol, infused drugs might be misclassified as therapeutic when they should be considered chemotherapy drug.
- Missing stop times – this can result in not being able to bill to the service’s full potential. If it’s a hydration service, it cannot be billed at all if it has a missing stop time.
- Assigning the wrong type of code for the drug that was administered
Potential revenue you’re leaving on the table
Medaptus only audits a small number of samples, but imagine if you audited all your charges? How much revenue are you missing out on? Learn more today.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.


