

We looked at data from over 30 hospitals in the U.S. to uncover:
- Who is typically responsible for the morning patient assignment and distribution processes?
- Which factors are most important to them when creating rounding lists? How many hospitals prioritize geography over continuity of care? How many evenly balance patients amongst hospitalists?
- What unique ways are hospitals creating their patient assignments that we can learn from?
These hospitals are all using Medaptus’ patient assignment software, Assign, to automatically create their daily rounding lists according to the criteria that is most important to them. Let’s dive in to see how they do it – and why.
Overview of Who We Analyzed
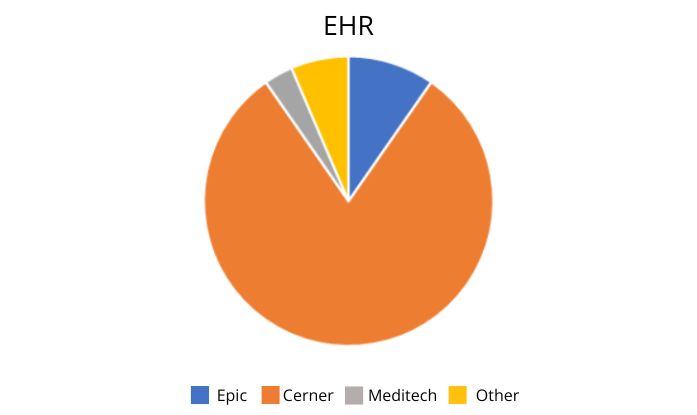
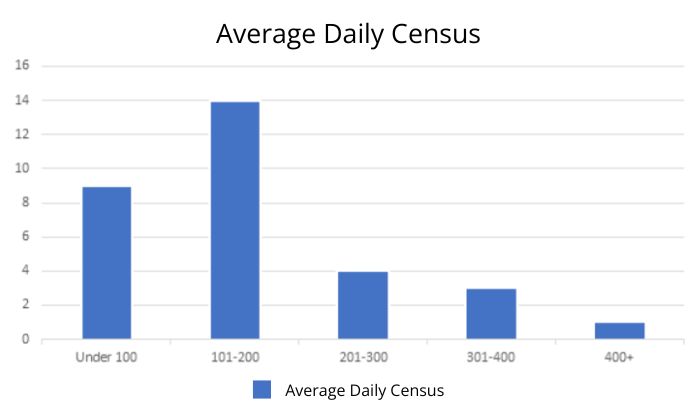
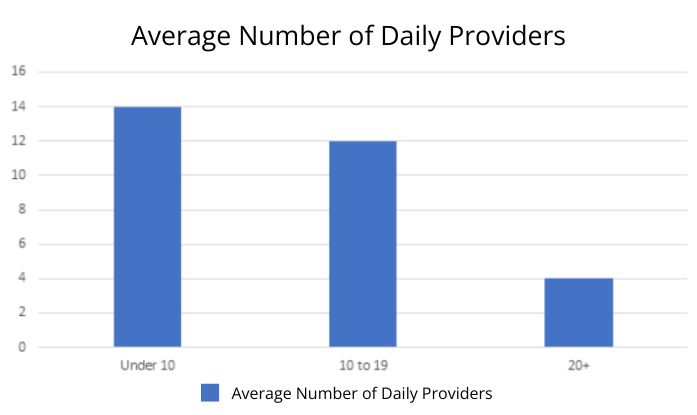
We analyzed 30 different hospitals in the U.S. to learn more about their hospital medicine team and patient assignment processes. Of the hospitals we analyzed, the majority use Cerner as their EHR and have a wide range in terms of their average daily census and daily providers.
Who is Responsible for the Morning Patient Assignment and Distribution Process?
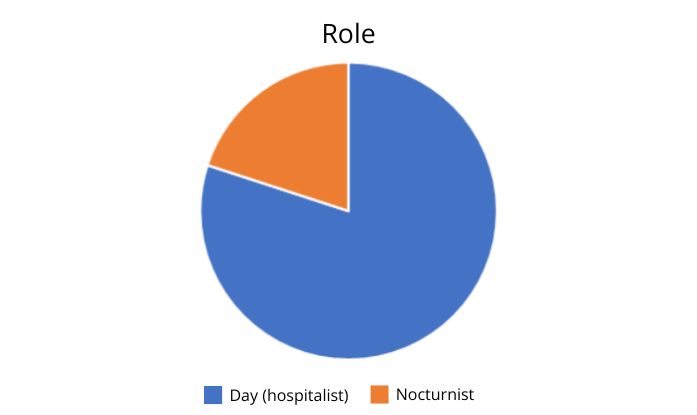
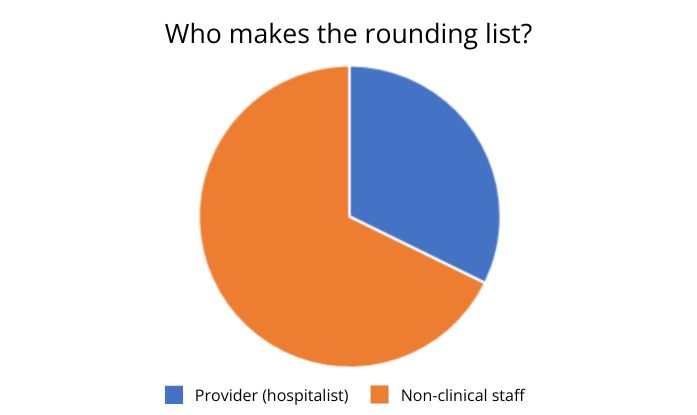
Our customers use Assign, our automated patient assignment software, to automate the process of assigning patients to providers every morning. Since the software takes the work out of the hospitalists’ hands, hospitalists don’t have to spend time making the list but typically just approve it. The majority of our customers sampled choose to reduce the burden on hospitalists and have non-clinical staff finalize the rounding list.
Most importantly, only one individual is involved in the rounding process, and for just a few minutes a day. In fact, we found that, on average, only 2-4% of patients are manually moved once assigned, and all other patients can be automatically assigned using Assign, with the rules pre-set by the organization.
How many staff members does your organization have to involve in patient distribution and how much time do they spend on it?
What is the ideal number of patients per provider?
Most of the hospitals we sampled aimed to assign a maximum of 15 patients per provider, on average. This varies for hospitals that also supplement with PAs and APPs, who can assist providers on rounding on their patients when there’s a higher volume.
“Studies show your ability to maintain the best metrics when you see more than 16 patients per shift quickly deteriorates and length of stay goes down and re-admission goes up,” said Dr. Kraydman. “Our ideal is 14-16 patients, but most days we are at 16-18 because the reality is, if you start your day with 16, you end up with 18 as downgrades, transfers, consults get assigned.”
Which factors do hospitals consider when distributing patients to providers?
The number one factor was to balance all patients evenly by provider. Almost every hospital in this analysis prioritized evenly balancing patients to providers, except for one (more on that one below). This is to ensure that providers see the same number of patients each day.
After they evenly balanced the number of patients, the other most common factor was geography: assigning patients to providers within a certain geographic range. For some hospitals, this might be limited to a certain floor, or tower. For others, they divided their hospital facilities into a “campus” and providers could only be assigned patients within a section of their campus.
“The big thing I’m surprised that the software was able to help us with was for doctors that aren’t available full-time, it’s very easy to make them 0.8 or 0.6 so the Assign software automatically gives them fewer patients. Before, people had to remember things like Dr. Nicholas is half-time today so give him half the patients as everyone else,” said Dr. Joseph Nicholas, Associate Chief of Medicine, Highland Hospital in Rochester, NY.
| Factors that Hospitals Prioritized for Distributing Patients Amongst Providers |
| Balance all patients evenly by provider. |
| Geographic rounding. |
| Balance by specialty or non-hospitalist groups (Cardio, urology, etc.). |
| Maintain continuity of care. |
| Adjust capacity for certain teams (some teams would have a higher maximum number of patients they could take, or a lower number if they had a lot of non-hospitalist responsibilities, such as a Director of Hospital Medicine). |
| Assign to a dedicated team for certain patient type, regardless of headcount. |
There’s much more to learn! Download our 2024 Patient Assignment and Provider Workload Benchmark Report to learn about the unique ways to assign and distribute patients, and improve the process at your organization.
Get the latest updates and news delivered to your inbox.
Subscribe to our newsletter today.


